Disclaimer
All content on Aidstat.com is created for healthcare professionals’ educational use only. It is not medical advice, or a substitute for clinical judgment, or patient/personal guidance. Always consult a qualified provider for diagnoses/treatment and verify practices with FDA/EMA/local guidelines. Aidstat assumes no liability for risks arising from the use of this information.
Chest Tube Size Calculator
Table of Contents
**Updates**
We updated this page on 27th of December 2025, added interactive Chest Tube Size Calculator and explainer on how the selector works. Added related questions to the FAQs section.
What is a chest tube and what conditions is it used for?
A chest tube drains air, blood, or fluid from around the lungs.
- Your lung sits inside your chest wall. Between them is a thin space called the pleural space. Normally this space has only a tiny amount of fluid.
Air, blood, or extra fluid can fill this space.
- When this happens, the lung cannot expand properly. This makes breathing difficult and can be dangerous. A chest tube drains the material out allowing the lung can to expand again.
Chest tubes are used for several conditions.
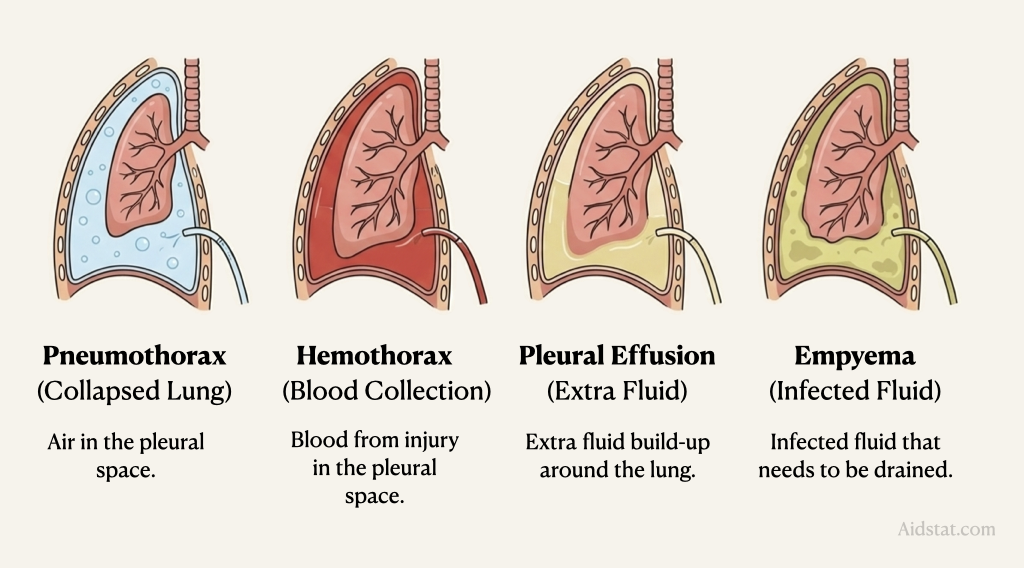
- Pneumothorax: Air in the pleural space (collapsed lung).
- Hemothorax: Blood in the pleural space from injury.
- Pleural effusion: Extra fluid building up around the lung.
- Empyema: Infected fluid that needs to be drained.
What is the French size system?
Chest tubes are measured using the French (Fr) scale.
- The French scale tells us the tube's thickness. It measures the outside width of the tube. Each French unit equals about 0.33 millimeters.
To convert French size to millimeters:
- Divide the French number by 3.
- Example: A 24 Fr tube is 8 millimeters wide.
- Calculation: 24 ÷ 3 = 8 mm.
A bigger French number means a wider tube.
- A 14 Fr tube is thin (about 4.7 mm).
- A 28 Fr tube is thicker (about 9.3 mm).
- A 36 Fr tube is very thick (about 12 mm).
Why does size matter?
- Smaller tubes are easier to put in and cause less pain. Larger tubes can drain thick fluid better. The right size depends on what needs draining.
What size chest tube do adults need?
Adult chest tube size depends on what is being drained.
- Adult rib spacing is similar across most people.
- We choose tube size based on the medical problem.
- Body size is less important in adults.
Small-bore tubes (14–22 Fr) are best for:
- Pneumothorax (air in the chest)
- Simple pleural effusions (thin fluid)
Why use small tubes when possible?
- They cause less pain when inserted.
- They are easier and faster to insert.
- They work just as well for air and thin fluid.
- They have fewer complications.
Medium-bore tubes (20–28 Fr) are best for:
- Hemothorax (blood in the chest)
- Pleural effusion with thick fluid
- Empyema (infected fluid)
Large-bore tubes (32–40 Fr) are rarely needed now:
- Older guidelines recommended these for all blood drainage.
- New evidence shows they don't work better, cause more pain and complications.
- Only use if smaller tubes fail, or for very thick clotted blood.
What size chest tube do children need?
Children need smaller chest tubes than adults.
- The size depends on the child's age or weight.
- Children's chest size changes as they grow.
- We use a formulas to find the right size.
Two formulas exist - they give the same answer:
Method 1: Direct Age Formula (Simpler)
Chest Tube Size (Fr) = Age (in years) + 16
Examples:
- 2-year-old: 2 + 16 = 18 Fr tube
- 6-year-old: 6 + 16 = 22 Fr tube
- 10-year-old: 10 + 16 = 26 Fr tube
Method 2: Rule of 4s (From ETT Size)
Step 1: Calculate ETT size = (Age ÷ 4) + 4
Step 2: Chest tube = ETT size × 4
- Example for 6-year-old:
- ETT = (6 ÷ 4) + 4 = 5.5 mm
- Chest tube = 5.5 × 4 = 22 Fr
Same as Method 1: 6 + 16 = 22 Fr
Both formulas have been validated in real patients.
- Tamatey formula (Age + 16): 106 children, zero complications.
- Rule of 4s: Widely used in pediatric emergency medicine.
- Both produce identical, safe sizing recommendations.
- Choose the method that's easier for you.
Doctors may adjust by 2 Fr up or down, adjustments based on the child's build and what needs to be drained.
How to use the chest tube size calculator
- Select patient type - Adult or Pediatric.
- Enter Age (for children) - You can also enter weight for more precision.
- Choose Clinical Indication - Select what needs to be drained.
- Click "Calculate" to get the recommended tube size range.
- If you need to redo, click "Reset" to start fresh.
**All information is private, no data is saved or shared.**
This calculator helps suggest chest tube sizes based on common clinical guidelines.
The recommendation is based on standard sizing practices used in hospitals and general ward settings.
Please note: actual tube size must always consider the individual patient’s anatomy, history, and clinical condition. Follow your local guidelines and always use your clinical judgement. This tool is a guide, not a replacement for professional judgement.
Chest Tube Size Calculator
Disclaimer
The online clinical calculators on Aidstat.com are for informational purposes only. They are not a substitute for clinical reasoning or professional judgment. They do not replace expert advice from qualified healthcare practitioners.
Extensive effort has been made to ensure accuracy and completeness. However, Aidstat.com cannot guarantee its accuracy or reliability. Users should independently verify any results from these tools. Always verify before making any medical or healthcare decisions.
Chest Tube Size Calculator
Get an evidence-based chest tube size recommendation
FAQs
Q1. What is the difference between pneumothorax and hemothorax?
- Pneumothorax is air in the chest space, causing lung collapse.
- Hemothorax is blood in the chest space, usually from injury, preventing lung expansion.
- Small cases may resolve alone; larger ones require a chest tube.
- Tube sizes differ: typically small (14–22 Fr) for air, medium (20–28 Fr) for blood.
Q2. What is pleural effusion and when does pleural effusion need a chest tube?
- It is excess fluid around the lung.
- Transudative (thin, from systemic issues like heart failure) often improves with treating the cause.
- Exudative (thicker, from infection or cancer) usually requires drainage with a tube.
- A chest tube is needed if breathing is difficult, fluid is infected, the lung can't expand, or fluid recurs.
Q3. What is empyema and why does empyema need special treatment?
- It is a collection of infected pus around the lung, often following pneumonia.
- Antibiotics alone are insufficient; the thick pus must be physically drained.
- Treatment requires a chest tube (typically 14–24 Fr) and IV antibiotics.
- Without proper drainage, it can cause permanent lung damage.
Q4. Why do small chest tubes work well?
- Latest evidence shows small (14–22 Fr) and medium (20–28 Fr) tubes are effective for air and blood.
- They cause less pain and allow faster recovery compared to historical large tubes.
- Large tubes (32–40 Fr) are now reserved for very thick, clotted blood or after smaller tubes fail.
- Current practice uses the smallest appropriately sized tube for the condition.
Q5. When can a chest tube be removed?
- The lung is fully expanded on imaging with no significant air or fluid left.
- Daily drainage is low (often <200-400 mL/day) and fluid is not bloody or infected.
- There is no air leak (no bubbling in the water seal).
- The patient is clinically stable, with comfortable breathing and no signs of infection.
Q6. What are the risks of chest tube placement?
- Insertion risks include bleeding, lung puncture, pain, and rare organ injury.
- The most common complication is tube malposition.
- Post-placement risks include blockage, infection, or accidental dislodgment.
- Risks are reduced by using ultrasound guidance, sterile technique, and appropriate tube size.
Q7. How do you calculate paediatric chest tube size?
- Use either formula:
- Chest Tube (Fr) = Age (years) + 16
- Rule of 4s: [(Age÷4)+4] × 4.
- Both methods give the same result, derived from and tested in pediatric patients.
- The calculated size may be adjusted ±2 Fr based on the child's weight and body habitus.
- For neonates, use weight-based sizing (e.g., 8–12 Fr).
Q8. What happens if the chest tube is too large?
- It causes significantly more pain and tissue damage.
- Insertion risk is higher, with greater potential for vascular or organ injury.
- There is no clinical benefit; large tubes do not drain better or faster.
- Modern practice favors the smallest effective tube to reduce complications.
Q9. What is the "Triangle of Safety"?
- It is the standard safe zone for chest tube insertion on the side of the chest.
- Boundaries are the pectoralis major (front), latissimus dorsi (back), base of armpit (top), and nipple line (bottom).
- This area avoids major vessels, organs, and breast tissue.
- Ultrasound guidance is recommended when possible to further improve safety, especially in children.
References
- Anderson, D., Chen, S.A., Godoy, L.A., Brown, L.M. and Cooke, D.T. (2022). Comprehensive Review of Chest Tube Management: A Review. JAMA surgery, [online] 157(3), pp.269–274. doi:https://doi.org/10.1001/jamasurg.2021.7050. Link
- Gomez, L.P. and Tran, V.H. (2023). Hemothorax. [online] Nih.gov. Available at: https://www.ncbi.nlm.nih.gov/books/NBK538219/. Link
- Hernandez, M.C., El Khatib, M., Prokop, L., Zielinski, M.D. and Aho, J.M. (2018). Complications in Tube Thoracostomy: Systematic review and Meta-analysis. The journal of trauma and acute care surgery, [online] 85(2), pp.410–416. doi:https://doi.org/10.1097/TA.0000000000001840. Link
- Inaba, K., Lustenberger, T., Recinos, G., Georgiou, C., Velmahos, G.C., Brown, C., Salim, A., Demetriades, D. and Rhee, P. (2012). Does size matter? A prospective analysis of 28–32 versus 36–40 French chest tube size in trauma. Journal of Trauma and Acute Care Surgery, 72(2), pp.422–427. doi:https://doi.org/10.1097/ta.0b013e3182452444. Link
- International Emergency Medicine Education Project. (2019). Pediatric Tube Sizes - Infographic. [online] Available at: https://iem-student.org/2019/07/24/pediatric-tube-sizes-infographic/. Link
- Kulvatunyou, N., Bauman, Z.M., Zein Edine, S.B., de Moya, M., Krause, C., Mukherjee, K., Gries, L., Tang, A.L., Joseph, B. and Rhee, P. (2021). The small (14 Fr) percutaneous catheter (P-CAT) versus large (28–32 Fr) open chest tube for traumatic hemothorax: A multicenter randomized clinical trial. Journal of Trauma and Acute Care Surgery, [online] 91(5), p.809. doi:https://doi.org/10.1097/TA.0000000000003180. Link
- Merkle, A. and Cindass, R. (2020). Care Of A Chest Tube. [online] PubMed. Available at: https://www.ncbi.nlm.nih.gov/books/NBK556088/. Link
- Park, S., Shin, S.-W., Kim, H.-J., Byeon, G.-J., Yoon, J.-U., Kim, E.-J. and Kim, H.Y. (2022). Choice of the correct size of endotracheal tube in pediatric patients. Anesthesia and Pain Medicine, 17(4), pp.352–360. doi:https://doi.org/10.17085/apm.22215. Link
- Tamatey, M., MM Tettey, Edwin, F., Kow Entsua-Mensah, B Gyan, Okyere, I., IK Adzamli, Adomako, K., G Offei-Larbi, EA Aniteye, DA Kotei, EA Ofosu-Appiah, Amoah, K., Ibrahim, U., P Adinku, M Maishanu, J Awodi, Osei, E., Yao, N. and LA Sereboe (2023). A Formula for the Determination of Appropriate Chest Tube Size and Length of Insertion in Children. Postgraduate Medical Journal of Ghana, 12(1), pp.8–12. doi:https://doi.org/10.60014/pmjg.v12i1.307. Link
- Terada, T., Nishimura, T., Uchida, K., Hagawa, N., Esaki, M. and Mizobata, Y. (2020). How emergency physicians choose chest tube size for traumatic pneumothorax or hemothorax: a comparison between 28Fr and smaller tube. Nagoya Journal of Medical Science, [online] 82(1), pp.59–68. doi:https://doi.org/10.18999/nagjms.82.1.59. Link
- Umem.org. (2025). UMEM Educational Pearls - University of Maryland School of Medicine, Department of Emergency Medicine. [online] Available at: https://umem.org/educational_pearls/1400/ [Accessed 27 Dec. 2025]. Link
- Zolfaghari, E.J. and Lee, M. (2024). Chest Tube Insertion in the Neonate. [online] Nih.gov. Available at: https://www.ncbi.nlm.nih.gov/books/NBK604214/. Link